What is serous cystadenoma?
Serous cystadenoma is a benign neoplasm that is usually present either in ovaries or in pancreas. The cyst is usually unilocular, but it can be multilocular. Cysts are filled with clear, serous fluid[1].
Serous cystadenoma of ovary
SC of the ovary is usually benign lesion that develops on the surface of the ovary, but in 20-25% cases it can be malignant. Benign neoplastic cysts make up 60% of all benign ovarian tumors. Sometimes the cyst may appear solid, because it develops papillary epithelial growths. This type of cyst is most common in women between 40-50 years of age. In around 15-25% of the cases SC are bilateral- found in both ovaries.
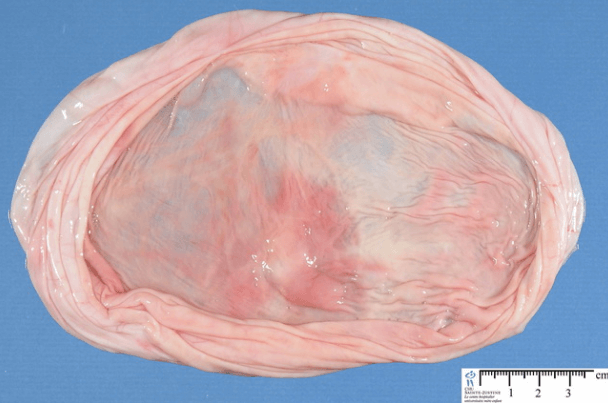
Cysts are around 3-10 cm large, oval or round shaped. The surface is smooth of the cyst is smooth. Fluid inside the cyst is usually clear or pale yellow[1,5]. 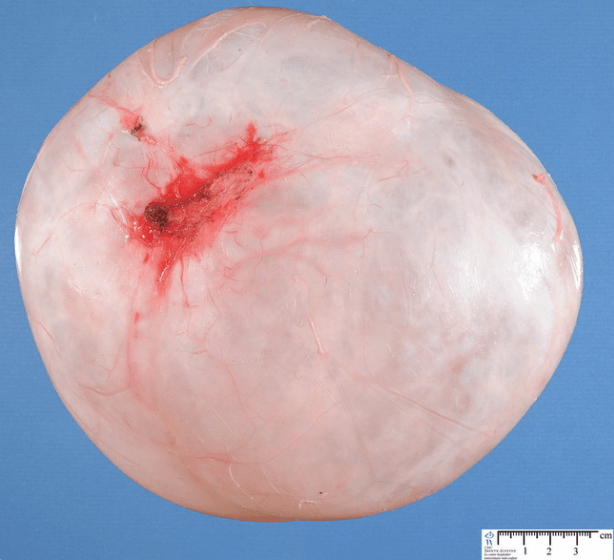
 Causes
Causes
Serous cystadenomas are caused by abnormal growth of the cells. This growth is not related to menstrual cycle. The exact causes are not known. There can be various genetic changes in these neoplasms, but certain mutations have not been found [1,5].
Clinical presentation
Usually cysts are asymptomatic and they are found incidentally doing routine gynecological examination. In some cases, especially when the cyst is large, they can cause symptoms, like:
- Abdominal bloating or swelling
- Pain in lower abdomen that can irradiate to lower back or thighs.
- Pain during intercourse
- Nausea, vomiting
- Changes in bowel movements- pain when passing stool or constipation
In case of torsion or rupture of the cyst, the symptoms can be severe:
- Fever
- Abdominal pain
- Rapid heart rate and breathing
- Vomiting
- Fatigue, dizziness or loss of consciousness [2]
Diagnosis
Clinical examination
Usually patients don’t have any complaints or they have unspecific symptoms. Larger cysts can sometimes be palpated during bimanual palpation. Complete medical history has to be acquired in order to exclude other possible conditions[5].
Laboratory studies
There are no specific laboratory findings that can lead to diagnosis of ovarian serous cystadenoma. In case the cyst has ruptured, signs of inflammation can found, such as elevated leukocyte count and C-reactive protein. To exclude possible malignancy, cancer marker tests can be performed. Ovarian cancer markers are:
- CA-125
- Human chorionic gonadotropin
- α-fetoprotein
To exclude the possibility of functional cysts (cysts that appear during certain period of menstrual cycle) or polycystic ovary syndrome, hormone levels (estrogen, testosterone) should be measured[1,5].
Histological examination
Since the cyst is filled with fluid, it is not safe to perform a biopsy. Usually the post-operative material is sent to laboratory for histological investigation.
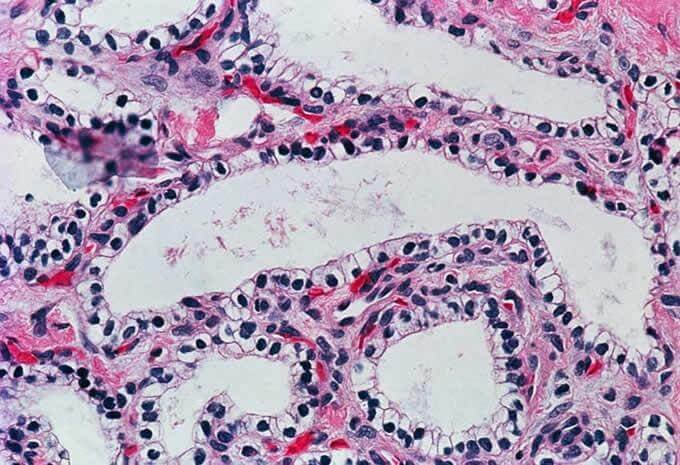
Cysts are usually localized in one ovary, but there can also be multiple cysts in one or both ovaries. The cyst is lined with single layer of epithelium- either columnar, ciliated epithelium similar to one found in fallopian tubes or cube-shaped cells similar to ones found on the surface of the ovaries. Cell space is filled with stroma rich in fibroblasts. Sometimes there might be papillae present in the cyst cavity. Sometimes there are actively proliferative, making the cyst seem solid [3].
Laparoscopy
Laparoscopy is both diagnostic and therapeutic technique. During laparoscopy the cyst can be visualized and surgically removed.
Imaging studies
- CT imaging can show a single or multiple fluid filled cysts with thin wall. Cysts can be large in size.
- Ultrasound- usually seen as a single cystic lesion on the surface of the ovary. The surface is smooth and cyst is filled with fluid. In some cases septations can be seen.
- MRI- usually a fluid filled cyst with thin wall. The image is usually homogenous. By using different MRI sequence it is possible to tell what kind of fluid is in it. Since serous cystadenomas contain clear, serous fluid, MRI imaging will show:
- T1- hypo-intense signal
- T2- hyper-intense signal
- T1 with contrast- enhancement of the cyst wall [4]

 Differential diagnosis
Differential diagnosis
- Functional cysts- follicle or corpus luteum cyst
- Polycystic ovary syndrome
- Endometrioma
- Malignant tumor of the ovary
- Colon tumor
- Diverticulitis
- Fallopian tube cancer
Treatment
If the cyst is small and causes no symptoms, no treatment is necessary. If the cyst is larger, causes symptoms or it is not sure if the cyst is benign or malignant, surgical removal is indicated. Since these cysts are mostly benign, no adjuvant treatment, like chemotherapy is necessary. Minimally invasive techniques are widely used to reduce the hospital stay and possibility of complications [5].
Serous cystadenoma of pancreas
Pancreatic serous cystadenoma is the most common benign lesion of the pancreas. These lesions occur in patients raging from 20 to 90 years of age, most commonly around 60 years. More than 60% of cases are found in women [6].
Causes
The exact cause of serous cystadenoma of the pancreas is unknown, but there are many risk factors:
- Old age
- Female gender
- Smoking
- Diabetes
- Positive family history
- Chronic pancreatitis
- Obesity
- Presence of genetic conditions:
- Hereditary breast and/or ovarian cancer syndromes
- Von Hippel-Lindau syndrome
- Peutz-Jeghers syndrome
- Lynch syndrome
- Multiple endocrine neoplasia type 1
- Neurofibromatosis type 1 [6,8]
Clinical presentation
Usually these lesions are asymptomatic, but cystadenomas larger than 4 cm can cause symptoms. Symptoms include:
- Abdominal pain that can irradiate to the back or shoulder blade
- Indigestion
- Loss of appetite
- In severe cases they can obstruct pancreatic ducts, causing jaundice and local damage of pancreas [6]
Diagnosis
Laboratory studies
There are no specific blood tests that could determine serous cystadenoma in the pancreas. In case the neoplasm is big and obstructs pancreatic ducts, increased serum amylase can be found. Large masses have to be differentiated from pancreatic cancer. Additional tests for cancer markers can be performed:
- Carcinoembryonic antigen
- CA 19.9
- CA 15.3
- α-fetoprotein[6]
Histological findings
The cysts have lining with cuboidal or flat epithelial cells. Usually these cysts in pancreas are multiple and smaller than 1 cm. Around 20% of cases they are microcystic- combination of small cysts creating a honeycomb-like appearance. Fluid in the cyst is clear[7].

![]()
![]()
Imaging studies
- CT- typical presentation is a multicystic mass in the head of pancreas. Sometimes calcifications can be seen.
- Ultrasound- nonspecific mass, sometimes the microcystic appearance can be distinguished.
- MRI- typical appearance is a cluster of small cysts with no communication with the pancreatic duct[8].

 Treatment
Treatment
Usually these lesions are asymptomatic and do not require any treatment. It is important to monitor the condition. If there are clinical symptoms, surgical removal of the cystadenoma is recommended and it is usually curative [6].
If you found this article helpful, share it on social media. For your personal experience use the comments box below.
References
- General information about SC of the ovary: http://www.dovemed.com/diseases-conditions/serous-papillary-cystadenoma-ovary/
- Symptoms of ovarian cyst: http://www.nhs.uk/conditions/Ovarian-cyst/Pages/Introduction.aspx
- Histological findings: http://www.pathologyoutlines.com/topic/ovarytumorserousbenign.html
- Imaging studies: https://radiopaedia.org/articles/ovarian-serous-cystadenoma
- General information and differential diagnosis of benign ovary cysts: http://patient.info/doctor/benign-ovarian-tumours
- General information about pancreatic SC: http://www.dovemed.com/diseases-conditions/serous-cystadenoma-pancreas/
- Histology of pancreatic SC: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1357749/
- Imaging studies in pancreatic SC: https://radiopaedia.org/articles/serous-cystadenoma-of-pancreas
Similar Posts:
- Ovarian Teratoma
- Stage 4 Pancreatic Cancer – Symptoms, Survival Rate, Life expectancy
- Brenner Tumor
- Krukenberg Tumor
- Germ Cell Cancer – Symptoms, Survival Rate & Prognosis
- Fallopian Tube Cancer – Symptoms, Prognosis, Survival Rate, Treatment
- Tumor Suppressor Genes





Leave a Reply