What is Klatskin Tumor?
Klatskin tumor is a type of cancerous growth develops at the junction between right and left biliary duct from where main bile duct is formed. All types of cancerous growth in the biliary duct are termed as cholangiocarcinoma. Among this almost 60% to 70 % biliary duct cancer is Klatskin tumor1,2.
History
Altemei, the great surgeon, and clinical educator first described the cancerous growth at the bifurcated junction of the biliary duct in 1957. Subsequently, Klatskin reported a series of 13 cases with a cancerous growth in the biliary junction and since then cholangiocarcinoma at the bifurcated area of the right and left biliary duct is known as Klatskin Tumor1,3.
Etiology
The etiology of the Klatskin Tumor is not evident based. Multiple pathological conditions, which cause acute or chronic ailments of the biliary tract may have the influence to develop a malignant growth. Some associated conditions which may influence the Klatskin Tumor growth are as follows:
Sclerosing cholangitis
It has been found that almost 40% of patients suffering from Klatskin tumor already have a history of primary sclerosing cholangitis, which is an inflammatory condition of the hepatic ducts. The idiopathic cause of the development of primary sclerosing cholangitis has a direct association of Klatskin Tumor.
Caroli’s disease
Some biliary cystic diseases are congenital, such as Caroli’s disease or choledochal cysts and almost 25% of Klatskin Tumor cases have an association with this condition.
Reflux of pancreatic secretions
An abnormal pancreatico-biliary duct junction, which possibly responsible for back flowing (reflux) of pancreatic secretions into the bile duct and may have an association with Klatskin tumor.
Parasitic infection
Opisthorchis viverrini and Clonorchis sinensis are chronic biliary tract parasitic infection and considered as a risk factor for the development of Klatskin tumor.
Stone formation in the bile duct
Choledocholithiasis and hepatolithiasis are the conditions which influence to altering the malignant changes.
Miscellaneous conditions
Apart from the above mentioned possible association, exposure to asbestos and nitrosamines or other industrial materials and the radiologic contrast agent like thorium dioxide (Thorotrast) are also a considerable risk factor for the development of Klatskin tumor 1,4.
Incidence Rate
Growing industrialization and other environmental factors may responsible for an annual increasing incidence rate of Klatskin tumor. The predominance of this disease mainly occur after six decades and that can extend up to eight decades of life. The incidence rate does not provide any gender bias-ness means both male and female have similar risk 1,5.
Sign and Symptoms
At the initial stage, Klatskin tumor is asymptomatic. But progression of the malignancy cause following symptoms:
- Abdominal pain
- Unexpected loss of weight
- General malaise
- Itchy skin (pruritus)
- Jaundice is in advance stage. After the onset of jaundice, the included symptoms are yellowish skin color, stools color changed to clay in color, as because of bile juice is responsible for normal stool coloration, dark yellow colored urine.
The metastasis of the Klatskin tumor can extend up to localized lymph nodes and from there malignancy can spread to pancreatic head, common hepatic artery, and portal vein6.
Diagnosis
The following are the different diagnostic tools use for Klatskin tumor diagnosis.
Laboratory tests
Laboratory test results provide following abnormalities, which indicates Klatskin tumor presence
- Considerable tumor marker for Klatskin tumor is Serum carbohydrate antigen (CA) 19-9. This marker is glycoprotein in nature and found to be high in blood serum of the affected individual.
- Elevated levels of conjugated bilirubin, alkaline phosphate (ALP) and gamma-glutamyl transpeptidase (GGT) are also observed7.
Ultrasound
- Ultrasound examination of the whole abdomen can provide some specific features of Klatskin tumor, which provides the following findings
- Intrahepatic biliary ducts images showed dilation, though similar findings are not present in the extrahepatic duct
- Right and left hepatic ducts are not united
- Tiny, solid lumps are present at the hepatic hilus and those may locally spread to the liver.
- It is considered that if no abnormality finds in the pancreas, as well as no tumor growth also present in the pancreatic region then further high degree accurate diagnosis is required for the Klatskin tumor8.
Biopsy
Endoscopic retrograde cholangiopancreatography (ERCP) is used to conduct biopsy for a suspicious mass present in the bile duct7.
CT Scan
Helical computerized computed tomography (CT) with contrast enhancement imaging tool is used for envisaging the spreading of the metastasis6.
Treatment and Management
The main aims of the treatment for Klatskin Tumor are biliary blockage breakage, resection of the tumor. Early stage diagnosis has some options to provide curative treatment for the Klatskin Tumor, which include chemotherapy and radiotherapy, surgical resection of the tumor. But the success of this treatment maximum depends upon the stage of the disease and treatment acceptance of the patient, as all these treatments have several side effects. But these treatments methods are not much effective in an advanced stage of Klatskin tumor when metastasis spread into a wide area.
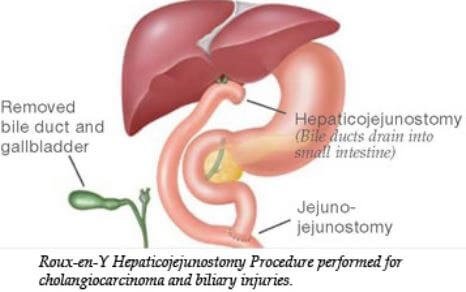
Surgical resection
Surgical resection is very carefully conducted so that negative margin of the tumor left over. Usually, liver surgical resection is conducted with caudate lobectomy and this process helps to provide the maximum prospect of negative resection margins.
Biliary stents
Biliary stents that may make with plastic and metal can place during palliative treatment.
Percutaneous transhepatic catheters
Percutaneous transhepatic catheters supply the greatest access for palliation of terminal Klatskin tumors.
Radiotherapy and/or chemotherapy
Radiotherapy and/or chemotherapy are the other treatment for non-operative Klatskin tumors. If resection is not possible then combination therapy of gemcitabin and cisplatin has been acknowledged as a standard Therapy6.
Survival rate
The survival rate of Klatskin Tumor is poorer as these tumors are only diagnosed at an advanced stage. In the case of unresectable tumors, then survival rate is minimum, whereas 25% of 30% surgical cases can survive up to five years6.
References
- Keith D Lillemoe; Klatskin tumors; Surgical Treatment: Evidence-Based and Problem-Oriented; Holzheimer RG, Mannick JA, editors; Munich: Zuckschwerdt; 2001; Online available at: https://www.ncbi.nlm.nih.gov/books/NBK6906/
- Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar cholangiocarcinoma. Ann Surg.(1992);215:31–38.
- Burke E, Jarnigan W R, Hochwald S N. et al. Hilar cholangiocarcinoma patterns of spread, the importance of hepatic resection for curative operation, and a presurgical clinical staging system. Ann Surg. (1998);228:385–394
- Hochwald S N, Burke E, Jarnagin W R, Fong Y, Blumgart L H. Association of preoperative biliary stenting with increased postoperative infectious complications in proximal cholangiocarcinoma. Arch Surg. (1999);134:261–266.
- Iwatsuki S, Todo S, Marsh J W. et al. Treatment of hilar cholangiocarcinoma (Klatskin tumors) with hepatic resection or transplantation. J Am Coll Surg. (1998);187:358–364.
- Junji Furuse, (2012); Klatskin tumor; Online available at http://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=EN&Expert=99978
- Weijing Sun (2006); Klatskin Tumor; OncoLink; Online available at https://www.oncolink.org/frequently-asked-questions/cancers/gastrointestinal/general-concerns/klatskin-tumor
- Meyer DG, Weinstein BJ.; Klatskin tumors of the bile ducts: sonographic appearance; Radiology. 1983 Sep;148(3):803-4; https://www.ncbi.nlm.nih.gov/pubmed/6308710
Similar Posts:
- Cholangiocarcinoma
- Duodenal Cancer – Symptoms, Prognosis, Survival Rate and Treatment
- DCIS Breast Cancer
- Krukenberg Tumor
- Urethral Cancer
- Stage 4 Liver Cancer (End Stage) – Life Expectancy, Survival Rate
- Choroidal Melanoma





Leave a Reply