What is Liposarcoma?
Liposarcoma is a malignant tumour made from neoplastic cells of fat tissue. They may develop in childhood, but more often in adulthood and it accounts for up to 28% of sarcomas of soft tissue in adults. The benign type of tumours of fat tissue is a lipoma, but malignant alteration froma lipoma to liposarcoma is very rare.

Symptoms
The signs are very unspecific. The tumour grows slowly in the muscles of the extremities, causing little or no symptoms at all. The slowly-growing mass doesn`t induce pain and may be firm or soft to touch. If the tumour is in the abdomen, it can grow up to 10 cm, without being noticed or before it begins to induce symptoms.
In time, a tumour may induce painful swelling, problems with blood flow through the veins (varicose veins are a consequence), due to compression, compression on the nerves with tingling, weakness of limbs and numbness, abdominal pain, nausea, vomiting, weight loss etc.
Symptoms are:
- Swelling and a growing lump that suddenly becomes painful,
- Nausea, vomiting, abdominal pain,
- Chest pain, coughing if the tumour is in the chest cavity,
- Problems with urination,
- Limited movements due to tumour mass, etc.
Three most common localisations are:
- Thighs,
- Retroperitoneum and
- Inguinal region (groin). (2)
Tumours in the retroperitoneum are the most dangerous since they can’t be diagnosed in time, and are difficultly visible on the ultrasound. They don’t induce any symptoms until they are large enough to compress other close structures.
Causes
Development and causes are unknown, although it is found that they develop from the deep fat tissue stroma and fat cells, and not from superficial subcutaneous fat tissue cells. Some scientists researched the genes that could be responsible for its development and they found an abnormality on the 12th and 13th chromosome, which are present in people with liposarcoma.
How many people have this tumour?
Liposarcoma appeas approximately in 2,5 per 1 000 000 people per year all around the world. More men than women have liposarcoma for unknown reasons. (1) (2) (3)
Types
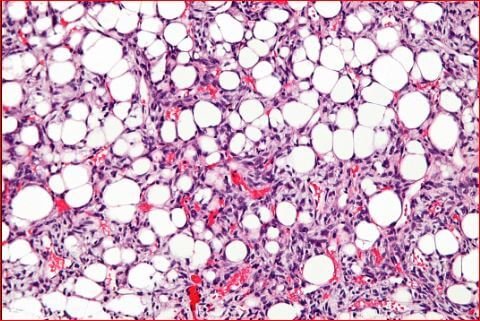
Well differentiated
Well differentiated liposarcoma is the commonest liposarcoma. Under a microscope, these tumours look very much like normal fat tissue. The cells are well differentiated which means that they share many cell characteristics with normal-functioning fat cell.
This speaks of good prognosis. Malignant alteration progresses slower than in other types. It is also a smaller chance for metastasing, however it can be locally destructive and aggressive.
Intraabdominal and retroperitoneal well differentiated tumours are associated with worse prognosis, no matter what size the tumour is. Tumour develops also in the thighs and groin. Dedifferentation of these tumours depends on various factor. Some of the well-differentiated liposarcomas are referred to as atypicalfor their tendency to change and act unpredictably. (4)
Myxoid
This type of tumour is intermediate in malignancy potential and aggression towards the tissue. It is very rare in our population. In 66% of cases, the tumours will develop in muscles of thigh.
The tumour is composed from fat-altered tissue and myxomatous stroma, developed from the mucoid tissue, which makes the tumour more soft in consistency and gelatinous.
This tumour is the second most commonly found liposarcoma, and one third ofpeople have this type. It looks similar to round-cell liposarcoma, but the latter has shown worse prognosis. Myxoid liposarcoma appears more frequently in young people, than other types. It is located in legs or very rarely in the retroperitoneum, in difference to well-differentiated type. (5)
Round cell
As previously mentioned, it is similar to myxoid liposarcoma, but, it is a high grade malignancy potentious tumour, with a high chance for metastasing. It is also known as a low differentiated myxoid liposarcoma. The tumour may be located in the thighs or abdomen.
Some myxoid tumours develop components of a round cells sarcoma, alterating their structure and increasing morbidity of the patient. Some scientists researched the transitional zones between these two types of tumour present at once, but it was concluded that only thepresence of a round cell sarcoma nd not some progenitory phase of it , speaks of worse prognosis. (6)
Pleomorphic
It is a rare type of tumour, which consists of cells that look different one from another. These cells are referred to as pleomorphic lipoblasts. This is a high-grade malignancy tumour, butfortunately is the rarest of tall 5 types. Histologically, the cells are polymorphic (spindle cell sarcoma), with presence of giant multinucleated cells.
In many cases, these tumours show necrosis and a very hign risk for metastazing. (7)
Malignant–Dediffierentiated
Dedifferentiated liposarcoma is the rarest type of liposarcoma. If a wel differentiated tumour shows malignant alteration, it will probably transform into a dedifferentiated liposarcoma. Most of the dedifferentiated liposarcomas are found in the retroperitoneum.
The characteristics of this tumour are atypical and unpredictable. They are sometimes a mixture of a low grade liposarcoma and a high grade spindle cell liposarcoma. Mostly, these tumours appear in elderly (older than 50). (8)
Diagnosis
Clinical exam won`t bring much information about the tumour type. Some genetical laboratory testings are necessary for that. CT and MRI imaging are useful to locate the tumour preciselyand its margins towards the surrounding tissue and can show the presence of metastases in the body.
Different types of liposarcoma appear differently onMRI, but the accurate histological diagnosis is set after the microscopic evaluation. It is performe after the biopsy.
Biopsy may be open or fine needle biopsy or aspiration. Staining is specific for liposarcoma (S100, Alpha 1 antitripsin ,desmins, myoglobin are evaluated in the microscope). Staging of tumour is specialistic task and consideres many factors of tumour and a patient. (3)
Prognosis
Prognosis is individually assessed. A 5-year survival is 100% in well differentiated liposarcomas, and 56% in pleomorphic liposarcomas. The location of the tumour is important, and usually the the abdominal tumours are difficult to diagnose and extract completely. That is why the relapses happen often in these cases.
Treatment
Surgery
Surgery and a complete resection on time, in most cases, no matter what subtype is, have excellent prognosis. However, for each liposarcoma a team of surgeons brings the decision about the treatment. The tumour is extracted along with a wide margin of surrounding tissue.
Sometimes there are indications for limb amputation, which happens to 5% of people with liposarcoma, any type.
Additional treatments
If the liposarcoma is high grade malignant the radiotherapy and chemotherapy are obligational. Radiotherapy prevented relapse of the disease in 90% of cases, and is recommended, opposing to chemotherapy which is rarely necessary, depending on the tumour spreading. The prognosis depends on the histological type. Myxoid variant in most cases demands radiation treatment, because of its aggressive nature. (2)
Works cited
- Liposarcoma. sarcomahelp.org. [Online] 2012. [Hivatkozva: 2017. 3 15.] sarcomahelp.org/liposarcoma.html.
- Liposarcoma symptoms and treatment. Medicinenet. [Online] 2016. [Hivatkozva: 2017. 3 15.] www.medicinenet.com/script/main/mobileart.asp?articlekey=184160.
- Schwartz. Liposarcoma RA. emedicine Medscape. [Online] 2016. emedicine.medscape.com/article/1102007-overview.
- Predicting survival for well-differentiated liposarcoma: the importance of tumor location. Smith CA, Martinez SR, Tseng WH, Tamurian RM, Bold RJ, Borys D, Canter RJ. 2012., J Surg Res 175(1).
- Myxoid liposarcom: a rare soft tissue tumor with a misleading benign appearance . Loubignac F, Bourtoul C, Chapel F. 2009., World Journal of Surgical Oncology 7(42).
- Myxoid/round cell liposarcoma of the extremitie. A clinicopathologic study of 29cases with particular attention to extent of round cell liposarcoma. Smith TA, Easley KA, Goldblum JR. 1996., Am J Surg Pathol 20(2).
- Pleomorphic liposarcoma: A clinicopathologic analysis of 19 cases . Downes KA, Goldblum JR, Montgomery EA, Fisher C, Path FRC. 2001., Mod Pathol 14(3).
- Dedifferentiated liposarcoma. www.tumorsurgery.org. [Online] [Hivatkozva: 2017. 3 15.] www.tumorsurgery.org/tumor-education/soft-tissue-tumor-types/dedifferentiated-liposacoma.aspx.
Similar Posts:
- Neuroendocrine Cancer – Symptoms, Treatment, Prognosis, Survival Rate
- Leiomyosarcoma – Survival Rate, Symptoms, Prognosis, Treatment
- Stage 4 Liver Cancer (End Stage) – Life Expectancy, Survival Rate
- PNET Tumor
- Solitary Fibrous Tumor
- Homer Wright Rosettes
- Pineal Gland Tumor





Leave a Reply