What is Granular cell tumor?
Granular cell tumor (GrCT) also known as Schwannoma or Abrikossoff tumor, is a rare soft tissue tumor derived from Schwann cells. Mostly these neoplasm´s are benign, but they can also be malignant. These tumors are of neural origin, and they are called granular cell tumors because of their appearance under the microscope. GrCTs are usually solitary, small neoplasms. They are usually located in the subcutaneous tissue, sometimes in submucosa, smooth or striated muscle. These tumors can also be found in internal organs, especially in the upper respiratory tract [2]. Another tumor of Schwann cells is Acoustic neuroma.
Schwann cells
Schwann cells or neurilemma cells are a part of peripheral nervous system. These cells are wrapped around axons and form the myelin sheath. Axon is a long and thin part of the nerve cell that conduce nerve impulses away from the cell. Myelin sheath prevents the loss of electrical impulse and increases the speed of impulse transfer [3].

 Benign Granular cell tumor
Benign Granular cell tumor
Usually granular cell tumors are benign. They can be found at various parts of the body, but most typical locations are the tongue, dermal and subcutaneous regions. These tumors are rarely found on the extremities. Benign tumors are easily removable and they have excellent outcomes. Usually GrCT occurs at age of 30-40 years, similar to Cowden syndrome.
Malignant Granular cell tumor
Malignant GrCT are very rare. Only around 0.5%-2% of GrCTs are malignant. In this case, they are very aggressive and have a poor prognosis. Malignant GrCT have a high risk of recurrence and metastasis. This type of tumor has a 40% mortality rate [4].
Causes & risk factors
There is no known cause for GrCT. This tumor is very rare and the exact statistics of its occurrence are not known. GrCT is more common in patients with African descent. In many cases GrCT occur as multiple lesions. Female gender is at higher risk of developing GrCT- female to male ratio is 3:2. GrCT is extremely rare in children- only 20 cases worldwide have been reported. It mostly occurs in middle age [2]. This syndrome is not known to be a part of other syndromes associated with higher risk of malignancies, like Li-Fraumeni syndrome.
Symptoms
GrCT are usually very slow growing singular or multiple nodules under the skin. The size is usually less than 3 cm in diameter. These nodules are not painful, but can be itchy or sensitive to touch. The skin over the lesion can be more pigmented or a bit red. Mostly these lesions are located in the head and neck area (70%). The most common location is the tongue. GrCT can also occur on the walls of larynx and trachea, intestines, breasts and anal region[2]. 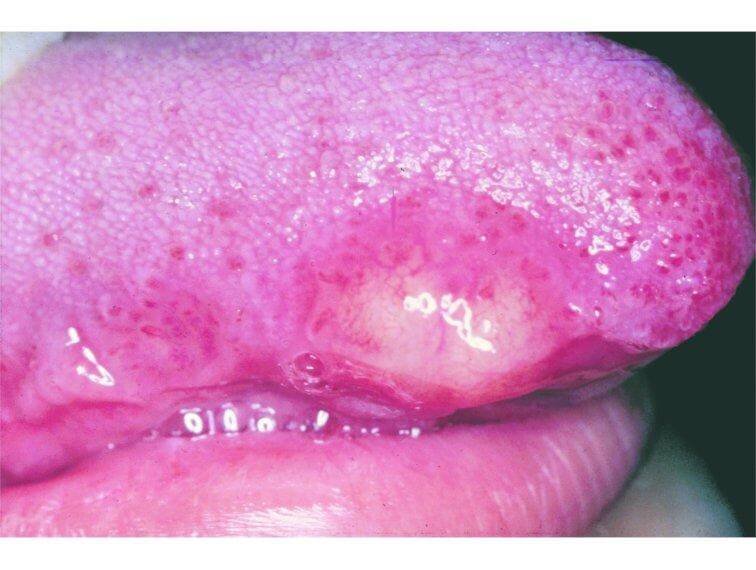
Diagnosis 
Diagnosis of GrCT consists of physical examination, laboratory findings and imaging studies.
Physical examination
Usually the lesions are small, less than 3 cm in size, solid. They usually grow with speed of 0.5-1mm per year (see other slow growing cancer: carcinoid cancer) . These lesions usually appear just beneath the epithelium. In oral cavity GrCT can obstruct saliva gland, which can cause pain [6].
Laboratory studies
There are no laboratory tests that can confirm GrCT. In case of malignant tumor tests should be one to determine organ function, for example liver enzyme tests, glomerular filtration rate. Also tests to exclude other possible conditions can be carried out [2, 6].
Histology
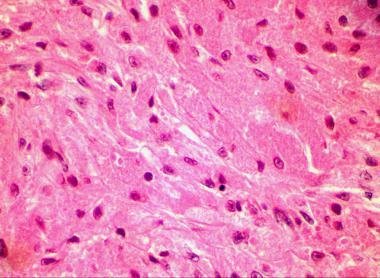
Only way to certainly diagnose GrCT is by histological examination of a biopsy sample.
The lesion is located in subdermal or submucosal tissue. It is not capsulated and has imprecise borders; sometimes these tumors invade adjacent tissue. It is formed from large uniform cells. It is now believed that the tumor is of neural origin. Tumor cells are large, polygonal and round shaped. Cells contain centrally located vesicular nuclei. Cytoplasm is granular. Cells are separated by small amount of connective tissue or sclerotic tissue. Sometimes the cells are arranged around nerve fibers [4].
![]()
Criteria for diagnosis
Since malignant GrCT has a high mortality rate it is very important to distinguish it from benign tumor. In 1998 Fanburg-Smith et al. established histological criteria of malignant GrCT:
- Necrosis
- Spindling
- Vesicular nuclei with large nucleoli
- Increased mitotic activity
- High nuclei to cytoplasmic ratio
- Pleomorphism
In addition, malignant lesions are usually larger – 4 to 15 cm. They can cause symptoms like pressure, pain, obstruction with following ulceration, hemorrhage and secondary infection. Malignant tumor can have metastasis, most commonly in regional lymph nodes and lungs, as well as other organs [1].
Immunohistochemistry
Immunohistochemistry is a method of detecting specific proteins by using specific antibodies that bind to specific antigens. Certain conditions can be diagnosed by finding the specific protein. In immunohistochemistry GrCT have positive protein S-100 and neuron-specific enolase. It can also be positive for myelin proteins and macrophage specific antigens (CD-68) [2, 5].

 Imaging studies
Imaging studies
Imaging studies can be used to detect tumor that is located in deep tissue or on visceral organs. Method of choice is magnetic resonance, but ultrasound imaging can also be used. Gastrointestinal neoplasms can sometimes be seen in endoscopy (also see hereditary polyposis syndrome) [7]. 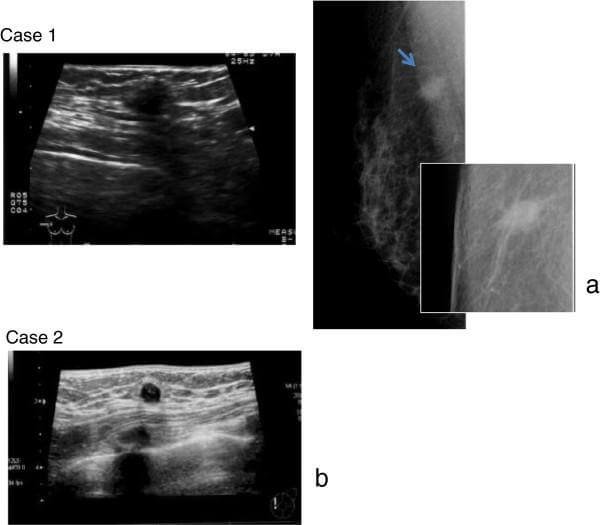
Differential diagnosis
Differential diagnosis of GrCT includes:
- Squamous cell carcinoma (if located in pharynx, tongue or vulva)
- Breast carcinoma
- Rhabdomyosarcoma
- Paraganglioma
- Oncocytic tumor
- Melanoma (also see Sezary syndrome) [2, 4]
ICD10 Code
The international classification of diseases and related health problems is a medical classification of all diseases from World Health Organization. GrCT is classified with code D10.1- Benign neoplasm of the tongue [8].
Treatment
The only way to treat GrCT is surgical excision of the lesion. Usually the results are very good, but recurrence is possible even if the tumor is resected with clear margins. Usually large en block resection is performed, because the tumor has imprecise borders. Malignant tumors have a higher risk of recurrence.
If malignant tumor is suspected, wide local resection is performed and adjuvant radiation therapy can be performed. In some cases chemotherapy is also used (read about adverse effects of chemotherapy and radiation therapy in myelodysplastic syndrome). Since malignant GrCT are very rare, there are no clear guidelines of their treatment, but method of choice remains tumor resection and close observation or recurrence [4].
If you find this article helpful, share it to others on social media. For your comments and personal experience use the comments box below.
References
- Thomas RM, Malignant granular cell tumor: a case report and re-evaluation of adverse prognostic features; available at: http://dx.doi.org/10.5430/crcp.v1n2p135
- General information about GrCT for patients and health specialists: http://emedicine.medscape.com/article/282430-overview
- Neural cells information: https://www.ncbi.nlm.nih.gov/pubmedhealth/PMHT0025728/
- Malignant GrCT, treatment: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4582131/
- Localization and histology of GrCT: http://link.springer.com/chapter/10.1007/978-3-7091-3846-5_82#page-1
- Diagnosis of GrCT:https://diagnosticpathology.biomedcentral.com/articles/10.1186/s13000-015-0357-2
- Imaging of GrCT: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2853648/
- ICD- 10: http://www.icd10data.com/ICD10CM/Codes/C00-D49/D10-D36/D10-/D10.1
Similar Posts:
- Mast Cell Tumor
- Brenner Tumor
- Squamous Cell Carcinoma in Situ – Pictures, Treatment, Symptoms
- Inoperable Brain Tumor
- Langerhans Cell Histiocytosis
- Clear Cell Sarcoma
- Nerve Sheath Tumor





Leave a Reply